
Abstract
PURPOSE We sought to determine the prevalence of airway obstruction and bronchodilator responsiveness in adults consulting for acute cough in primary care.
METHODS Family physicians recruited 3,105 adult patients with acute cough (28 days or shorter) attending primary care practices in 12 European countries. After exclusion of patients with preexisting physician-diagnosed asthma or chronic obstructive pulmonary disease (COPD), we undertook complete case analysis of spirometry results (n = 1,947) 28 to 35 days after inclusion. Bronchodilator responsiveness was diagnosed if there were recurrent complaints of wheezing, cough, or dyspnea and an increase of the forced expiratory volume in 1 second (FEV1) of 12% or more after bronchodilation. Airway obstruction was diagnosed according to 2 thresholds for the (postbronchodilator) ratio of FEV1 to forced vital capacity (FEV1:FVC): less than 0.7 and less than the lower limit of normal.
RESULTS There were 240 participants who showed bronchodilator responsiveness (12%), 193 (10%) had a FEV1/FVC ratio of less than 0.7, and 126 (6%) had a ratio of less than the lower limit of normal. Spearman's correlation between the 2 definitions of obstruction was 0.71 (P <.001), with discordance most pronounced among those younger than 30 years and in older participants.
CONCLUSIONS Both bronchodilator responsiveness and persistent airway obstruction are common in adults without established asthma or COPD who consult for acute cough in primary care, which suggests a high risk of undiagnosed asthma and COPD. Different accepted methods to define airway obstruction detected different numbers of patients, especially at the extremes of age. As both conditions benefit from appropriate and timely interventions, clinicians should be aware and responsive to potential underdiagnosis.
INTRODUCTION
Undetected chronic obstructive lung disorders in primary care, such as asthma and chronic obstructive pulmonary disease (COPD), are common in high-risk patients (eg, smokers) who complain of acute cough.1,2 Cough is among the most common conditions for which people seek health care,3 and family physicians could help their patients by considering underlying asthma or COPD when their patients consult them for acute cough. Timely treatment improves quality of life and reduces future exacerbations of these underlying conditions.4,5
Our searches identified only 2 relevant studies describing the proportion of underlying obstructive lung disorders in patients consulting their family physician for cough. Thiadens and colleagues6 included 192 patients (mean age of 44 years) consulting their family physician for cough persisting for at least 14 days; 74 were given a diagnosis of asthma (39%), and 14 were given a diagnosis of COPD (7%). Broekhuizen and colleagues7 included 353 patients (mean age of 63 years) with cough lasting more than 14 days, 23 of whom were given a diagnosis of asthma (7%) and 102 were given a diagnosis of COPD (29%). Both studies were relatively small and the mean duration of cough in the latter study was long (93 days). More frequent visits and persistent cough are known to be associated with diagnosis of COPD,8 whereas the relation with underlying obstructive airways disease and acute cough (≤28 days) has not previously been quantified.
We therefore set out to determine the prevalence of abnormal lung function results that could identify patients at high risk for a diagnosis of COPD or asthma in a large multicenter study of adult patients consulting their primary care physicians with acute cough.
METHODS
Ours was a cross-sectional prevalence study. Data were collected in 16 primary care research networks in 12 European countries participating in the Genomics to Combat Resistance Against Antibiotics in Community-acquired LRTI in Europe (GRACE) (http://www.grace-lrti.org) Network of Excellence. Participating family physicians recruited consecutive patients who were aged 18 years or older, with acute cough as the main symptom, and consulting for the first time for this disease episode. Although acute cough is usually defined as fewer than 21 days, some studies have shown that cough can last more than 3 weeks.9 We therefore decided to adopt the broader inclusion criterion of 28 days or less for acute cough. Nonwhite patients were excluded because of ethnic differences in lung function reference values.10 Other exclusion criteria for this analysis were diagnosis of asthma or COPD in the clinical record at the time of the index consultation and serious causes of compromised immunity. All patients provided written informed consent, and the study was approved by the medical ethics committees of all participating centers.
Measurements
Family physicians recorded the participants' history (eg, current complaints, comorbidity, medications) and findings from the physical examination on a standardized case report form. Spirometry was performed according to a strict protocol between day 28 and 35 after inclusion with the aim of obtaining results during a stable phase.4,11 Staff in the participating primary care centers underwent standardized training in spirometry. Measurements included the forced vital capacity (FVC) and the forced expiratory volume in 1 second (FEV1) before and at least 15 minutes after bronchodilation with 400 mg of salbutamol. The best of a minimum of 3 acceptable retained flow volume curves was used to determine the postbronchodilator FEV1:FVC ratio.4
Diagnostic Outcome
Bronchodilator responsiveness was diagnosed if recurrent (more than 1 other episode in the past year) wheezing, cough, or chest tightness were present (patient reported) in combination with an increase in FEV1 of at least 12% or more than 200 mL after bronchodilation. Persistent airway obstruction was diagnosed on the basis of the postbronchodilator FEV1:FVC ratio. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD), a ratio of less than 0.7 confirms COPD.4 Because the FEV1:FVC ratio physiologically decreases with age, however, there is controversy about using a fixed threshold to define obstruction4,12; others base a definition of obstruction on the lower limit of normal (LLN) of the FEV1:FVC ratio according to sex and age.13 The presence of airway obstruction in our study was defined by both methods: (1) a fixed FEV1:FVC ratio of less than 0.7 according to GOLD (obstruction GOLD), and (2) FEV1:FVC ratio of less than the LLN according to the European Respiratory Society guidelines (obstruction LLN).14 Correlation between the 2 definitions was calculated with Spearman's rank correlation coefficient.15
Data Analysis
Only participants with complete spirometry results were included in the present analysis. For the included participants, missing results (apart form spirometry) were imputed using multiple regression techniques. Data were analyzed using SPSS 17.0 for Windows (SPSS Inc) and R 2.8.1 (R Project for Statistical Computing).16 The prevalence of asthma, COPD GOLD, and COPD LLN was calculated for the entire study population and for subgroups of age, sex, and smoking history (current, past, never). These groups were compared using χ2 tests.
RESULTS
Patient Characteristics
Family physicians recruited 3,105 participants with acute cough. Participants with preexisting physician-diagnosed (according to the physicians' medical fi le) asthma (n = 329), physician-diagnosed COPD (n = 183), those who were of nonwhite ethnicity (n = 87), and those who had incomplete spirometry results (n = 585) were excluded, resulting in 1,947 participants for the analysis (Figure 1).10 Less than 0.1% of history items, 1% of physical examination items, and 12% of diary data were missing (Table 1). In some countries, spirometry measurements were available for only a minority of participants (eg, Italy and Slovakia, Supplemental Appendixes 1 and 2, available at http://annfammed.org/content/10/6/523/suppl/DC1). There were no important differences between study participants with and without spirometry results, apart from mean age (46 years for those without spirometry, data not shown). The mean age of the study population was 50 years (SD = 16 years), 40% (n = 770) were male, mean height was 168 ± 9 cm, and mean weight was 76 ± 16 kg. Mean duration of cough before consultation (9 days) and average day of recovery (12 days) were similar in participants with and without undetected asthma or COPD.

Flowchart of the study and participants.
Prevalence of Obstruction and Reversibility
Of the 1,947 participants, 240 met our diagnostic criteria for bronchodilator responsiveness (12%), of whom 193 showed a FEV1 increase of both 200 mL and 12%; 193 (10%) had airway obstruction GOLD and 126 (6%) had airway obstruction LLN (Spearman's ρ = 0.71, P <.001). Of the participants with obstruction GOLD and LLN, 92 and 6 7, respectively, reported recurrent respiratory symptoms (more than 2 cough episodes or had awakened with more than once with chest tightness last year).
In total, 202 (10%) participants met obstruction criteria according to at least 1 of the 2 definitions, and 41 participants showed both bronchodilator responsiveness and obstruction (2%) (Table 1). Of the 193 participants with obstruction GOLD, 86 cases (45%) had an FEV1 above the 80% predicted according to age, sex, and height; 84 (44%) had an FEV1 between the 50% and 80% predicted; 17 (8%) had an FEV1 between the 30% and 50% predicted, and 6 (3%) had an FEV1 of less than the 30% predicted.
The prevalence of bronchodilator responsiveness and airway obstruction (GOLD or LLN) varied largely per country and was related to the proportion of known asthma and COPD (Supplemental Appendix 2, available at http://annfammed.org/content/10/6/523/ suppl/DC1).
The prevalence of bronchodilator responsiveness was 15% in participants younger than 50 years and 11% in participants aged 50 years and older (P = .004), 14% in male and 12% in female participants (P = .18), 11% in never or past smokers, and 16% in current smokers (P = .02). In participants with duration of cough shorter than 14 days at the first consultation, the prevalence of reversibility was 12% and 14% if duration was 14 days or longer (P = .20, Table 2).
The prevalence of obstruction (GOLD or LLN) was 6% in participants younger than 50 years and 14% in participants aged 50 years and older (P <.001), 11% in male and 10% in female participants (P = .75), 9% in never smokers and 10% in past and 13% in current smokers (P = .10). In participants with cough for fewer than 14 days at the first consultation, obstruction was found 10%; in those with complaints longer than 14 days, it was 11% (P = .82, Table 2).
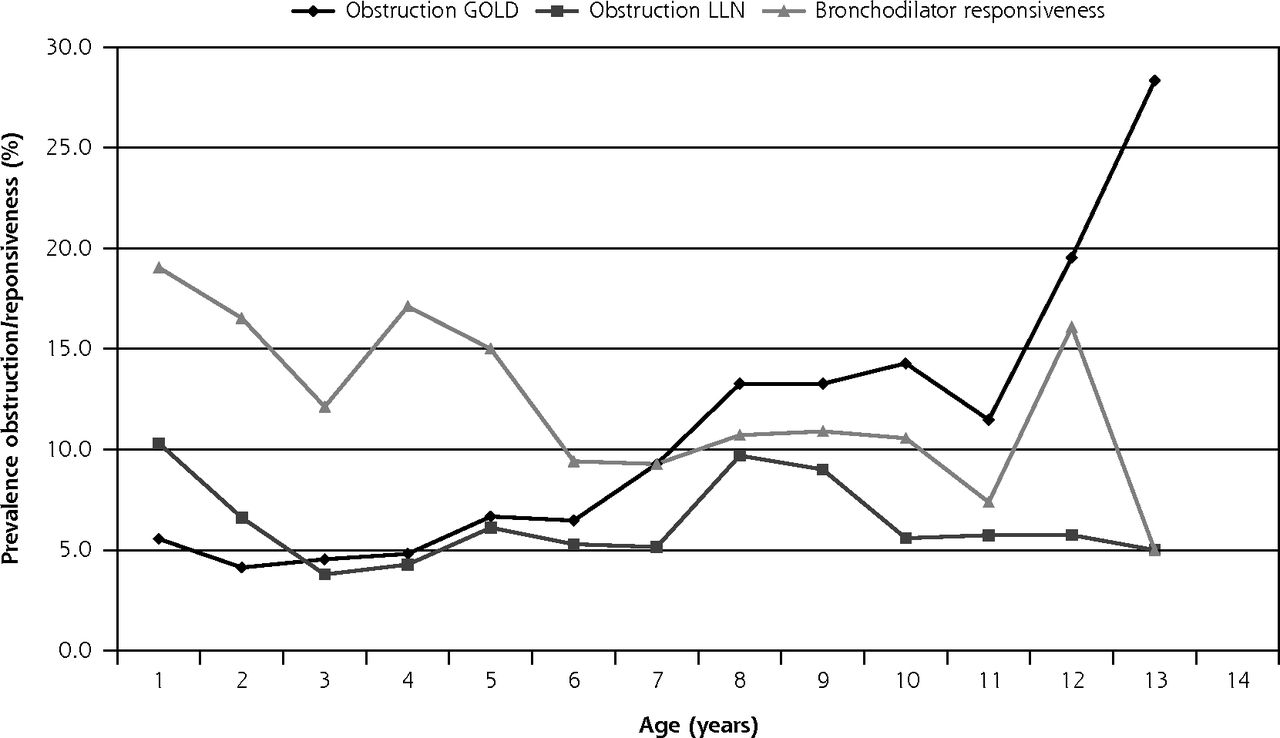
More participants showed obstruction GOLD than LLN, apart from in the under-30-year age-group, with the discordance highest in participants aged older than 50 years (14% vs 7% for airway obstruction GOLD and LLN, respectively (Figure 2).
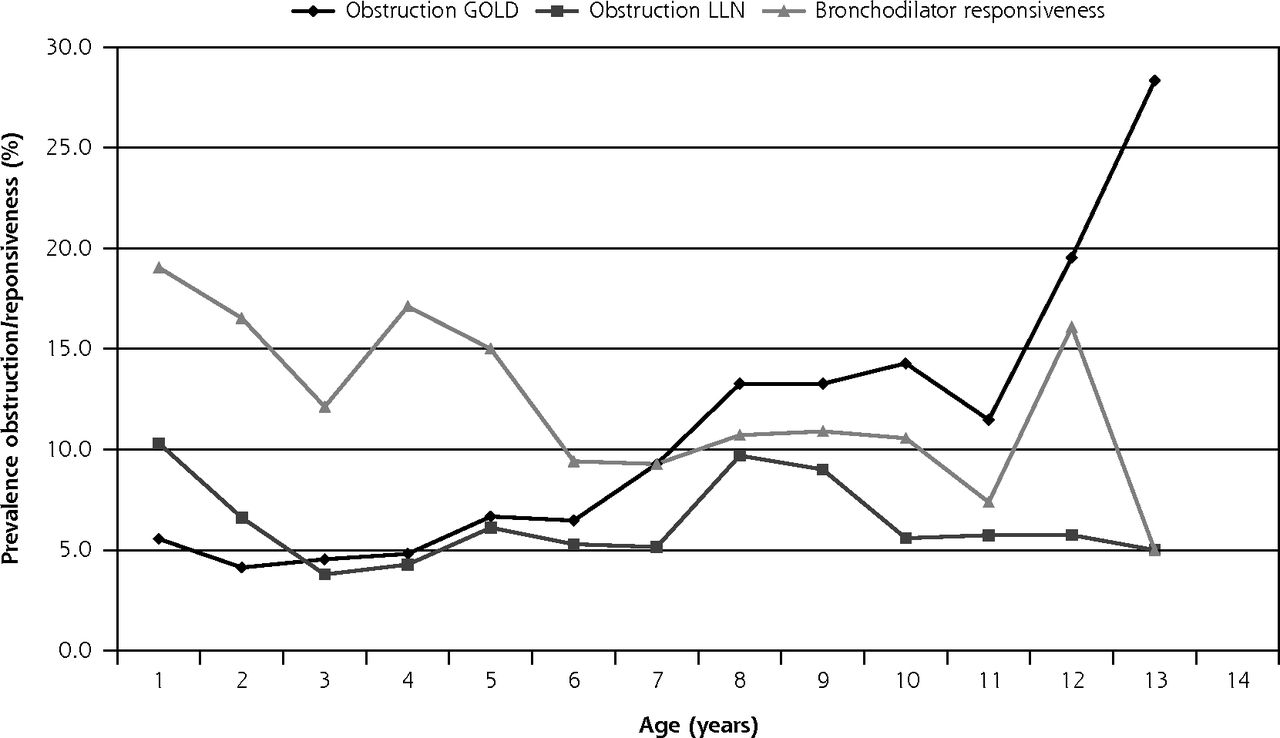
Prevalence of airway obstruction and bronchodilator responsiveness in patients consulting for acute cough, by diagnostic definition and age-group.
ERS = European Respiratory Society; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; GOLD = Global Initiative for Chronic Obstructive Lung Disease; LLN = lower limit of normal.
Note: obstruction GOLD = according to the GOLD defi nition: FEV1:FVC less than 0.70. Obstruction LLN = according to ERS: LLN of FEV1:FVC ratio for male patients: −0.18 × age + 87.21 − (1.64 × 7.17); for female patients: −0.19 × age + 89.10 − (1.64 × 6.51).
DISCUSSION
Main Findings
In adult patients without preexisting physician diagnosed asthma or COPD who consulted for acute cough in primary care and who underwent pre- and postbronchodilator spirometry 4 weeks later, 13% showed bronchodilator responsiveness, together with a history of recurrent airway symptoms. People with repeated episodes of acute cough and reversible airway obstruction may have undiagnosed asthma. Obstructive spirometry according to the GOLD definition was present in 10% and according to the LLN definition in 6% of the patients. The GOLD definition classified more participants with an obstructive condition than did the LLN definition, especially among older participants. Although these findings are necessary but not sufficient to diagnose COPD and asthma, patients with these findings are at higher risk of having (yet undetected) chronic obstructive lung disease and might benefit from ongoing treatment.
Strengths and Limitations
We studied a clinically relevant population, namely, those consulting their family physician for respiratory complaints (acute cough), whereas most previous studies included only asymptomatic volunteers (open-population studies).17-19 Moreover, we studied the prevalence of lung function abnormalities in 12 European countries, whereas most other studies were from a single country. Reviews mention considerable variation in reported prevalence of obstructive lung disease, attributed to differences in risk exposure, population characteristics, methods, and definitions used to measure disease.18,20 In our pan-European study, standardized measurements were used, and population differences were taken into account in analyses, increasing generalizability of the results. Finally, we measured spirometry results 4 weeks after an index consultation, when most acute episodes of cough had resolved.
A limitation of our study is that a formal clinical diagnosis of asthma and COPD could not be established within our research design. We were merely able to identify those with high risk of these disorders. Persistent airway obstruction is a hallmark of COPD (but can also develop in asthma, especially in smokers), and bronchodilator responsiveness suggests asthma and is common in COPD. There is no single reference standard to diagnose asthma and COPD; these diagnoses should be based on clinical history and physical examination combined with spirometry results. Repeat spirometry and additional tests, such as body plethysmography for COPD and histamine- or methacholine-provocation tests for asthma, can increase diagnostic certainty. We therefore considered that the diagnostic categories we used (bronchodilator responsiveness and airway obstruction) were most appropriate for reporting our results. Diagnostic certainty in our identified study participants could also have been be increased by specific questionnaires for asthma and COPD; however, the diagnostic value of such questionnaires is uncertain. Our findings reinforce the need for more objective criteria to define asthma or COPD.
The differences in prevalence of airway obstruction and bronchodilator responsiveness that we found between countries might represent real differences, possibly caused by variation in air pollution or demographic characteristics. Moreover, the differences could also partly be explained by varying definitions and guidelines between countries, because an active detection policy for asthma and COPD reduces the number of undetected cases (Supplemental Appendix 2). A further limitation of our study is that differential patient selection (selection bias) between countries cannot be excluded, as we were not able to gather data on the eligible participants who were not included in the study. Another problem is the high number of missing or incomplete spirometry results for some countries (eg, Italy, Supplemental Appendixes 1 and 2), resulting in unreliable prevalence estimates in those countries. We did not record whether missing spirometry data (19%) arose from uninterpretable results or whether spirometry was not performed in these patients. Moreover, there was no additional standardized reassessment of all spirometry curves in our study, and the individual judgment of quality by the individual research staff members may have led to misclassification.
Participants were assessed using the equipment already available in the participating practices and so were assessed using a range of models and makes of spirometer (list available on request). Spirometry was performed according to a uniform protocol at all study sites, however, and all general practice staff members performing spirometry were trained to analyze spirometry curves. A primary care study has shown that spirometry tests in a primary care setting conducted by staff with adequate training are comparable in quality to pulmonary function laboratory measurements.21 Finally, participants were included who were using inhaled lung medication, which may have influenced their spirometry results. Even so, it is common for primary care patients to be treated with inhaled medication without first undergoing diagnostic work-up for asthma or COPD.
Comparison With Other Studies
The prevalence of abnormal spirometry patterns in our study was lower than in other studies. The diagnostic outcomes we used, however, differed from those used in these previous studies. Thiadens and colleagues6 found asthma in 39% and COPD in 7% of the cases, and Broekhuizen and colleagues7 found previously undetected COPD in 30%. Apart from the older age of participants in Broekhuizen's study, the most likely explanation is that the average duration of cough was shorter in our study (8.7 days, with a self-reported recovery rate of 70% at 14 days). In an open-population study of the presence of chronic lung diseases in 169 smokers, 18% had COPD, increasing to 27% among those with chronic cough.1
There was no notable variation in prevalence of airway obstruction among nonsmokers (9%), past-smokers (10%), and current smokers (13%) in our study, which is possibly related to the large number of missing results on smoking status. Alternatively, smokers may have been more likely to have had COPD previously diagnosed.
Studies in the general population found prevalence of obstructive lung disease that varied from 23% to 29%, depending on diagnostic criteria.17-19 Likewise, findings from our study show that differences in age, sex, smoking status, and geographical population, as well as the definition that is used, can result in systematic differences in international prevalence rates. The increasing airway obstruction GOLD prevalence with older age, ie, when using the fixed ratio, is in line with recent warnings for overdiagnosis of airway obstruction in older adults. Also, the higher prevalence according to the LLN definition in younger participants is consistent with previous studies.13
Clinical Implications and Conclusions
An important proportion (approximately one-fifth) of adult patients without an established diagnosis of asthma or COPD consulting their family physician with acute cough showed subsequent airway obstruction or bronchodilator responsiveness, which suggests undetected asthma or COPD. Given effective pharmacological and lifestyle modification interventions, especially interventions to assist in quitting smoking, identifying and providing appropriate treatment and advice to these patients is likely to improve their quality of life and reduce exacerbations. Moreover, an accurate diagnosis could help to motivate smokers to quit.22 Finally, detection of asthma and COPD may help to reduce unnecessary use of antibiotics in patients with acute cough, because a noninfectious cause (obstruction) will also be considered.
Different methods to define airway obstruction resulted in twofold differences in the prevalence estimates among participants aged 50 years or more. Our results from symptomatic patients seeking health care uniquely confirm findings from open-population studies that a fixed cutoff value of 0.70 (GOLD) should be used to define obstruction with caution in the extremes of age.12,13
Acknowledgments:
We would like to thank the entire GRACE team for their diligence, expertise and enthusiasm. Finally, we are indebted to all of the patients who consented to be part of GRACE, without whom this study would not have been possible.
Funding support: The design and conduct of the study, collection, management, analysis, and interpretation of the data and preparation, review, and approval of the study were all funded by 6th Framework Program of the European Commission (Reference: LSHM-CT-2005-518226). In Flanders (Belgium) this work was supported by the Research Foundation, Flanders (G.0274.08N).
Footnotes
-
Conflicts of interest: authors report none.
-
Disclaimer: The funding sources were not involved in the design, conduct, analysis, and interpretation of the data, or in the writing and decision to submit the manuscript. There was no pharmaceutical company involved. The corresponding author had full access to the data and had final responsibility for the decision to submit for publication.
-
Previous presentations: This work was presented at the WONCA congress (September 2011, Warsaw, Poland) and the ERS congress (September 2011, Amsterdam, the Netherlands).
-
To read or post commentaries in response to this article, see it online at http://www.annfammed.org/content/10/6/523.
- Received for publication September 7, 2011.
- Revision received March 1, 2012.
- Accepted for publication March 15, 2012.
- © 2012 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}